Leading Healthcare Companies: How Healthcare Enterprises Use GEA to Break Through Communication Dilemmas? From Single Point Content to Continuous HCP Awareness
Healthcare enterprises leverage GEA to integrate medical content, addressing issues such as content fragmentation and low reuse rates, enhancing communication efficiency, and transforming phase-based content production into a long-term medical awareness influence system.
For many healthcare companies, the issue of medical communication is often defined as a content production problem: Is the material rewriting done properly? Are the channels sufficiently covered? Are compliance requirements met?
An innovative pharmaceutical company has been following this path for a long time while promoting a chronic disease management product's market education. They have the materials, expert consensus, and content team—yet they have always struggled to answer a truly critical question: Why is it that despite a considerable amount of content produced, the cognitive influence on doctors and patients remains difficult to sustain?

After reinterpreting this issue, they realized they were actually facing something else: content production was about "completing a single communication," while what the company truly needed to establish was "the capability structure that allows medical knowledge to continuously influence cognition." These two matters have never been the same question.

Limitations of Traditional Medical Content Systems: Content Exists, but the Communication Structure Has Yet to Be Established
This company faces a typical challenge in chronic disease management market education: high professional thresholds, complex audience stratification, long communication cycles, and the need for continuous content updates. There is no shortage of guideline interpretations, expert interviews, and academic conference materials, but these materials are fragmented and cannot form a coherent communication capability.
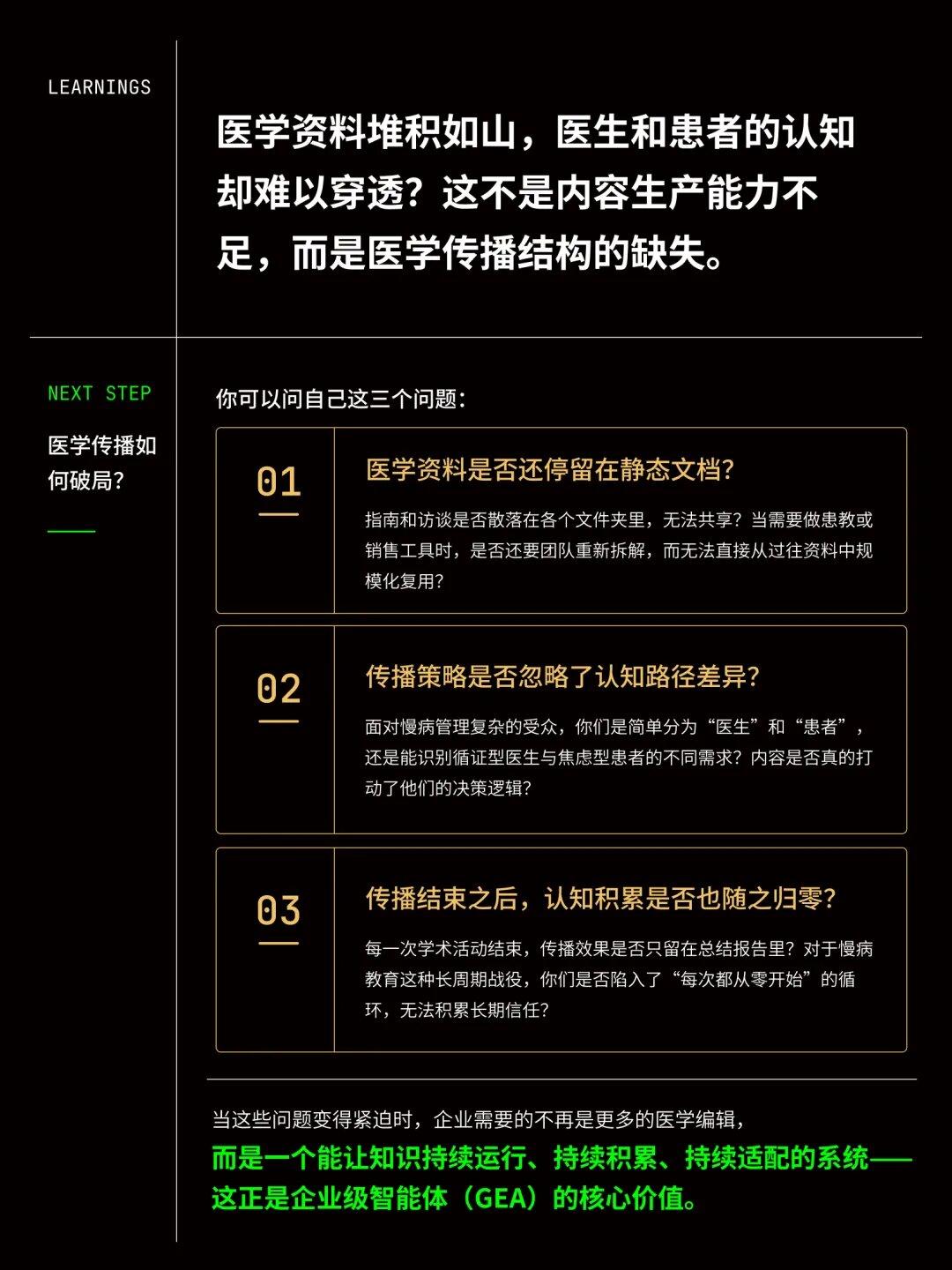
The core limitation of traditional medical content systems lies not in the quality of materials, but in the operational methods.
Content is initiated as a project, completed once and then published; the expression methods required by doctors, patients, and sales teams are completely different, but the underlying medical knowledge cannot be shared or reused; communication effects cannot be systematically accumulated, nor can they enter the next round of strategic adjustments. Each communication activity starts anew from nearly zero.
In a communication scenario like chronic disease education that heavily relies on long-term trust accumulation, this limitation is particularly evident. Doctors and patients do not receive a single piece of content, but rather a continuously emerging knowledge structure. One-time content investments struggle to produce lasting effects on the cognitive level.
Building Medical Communication Contexts, Turning Historical Materials into Callable Knowledge Assets
The guidelines, expert interviews, academic conference materials, and historical communication materials accumulated by the company have been uniformly organized into a structured medical communication context system. These contents, originally scattered across different communication nodes, have for the first time formed a basis for medical expression that can be continuously called upon, automatically adapted, and reused across channels. Medical materials are no longer static documents but have become a knowledge infrastructure that the system can continuously call upon.
The direct result is: the same set of medical knowledge can automatically generate different expression versions for doctors, patients, sales, and conferences without needing to recreate each time. The increase in content reuse rates begins to happen from here.

From Static Audience Labels to Dynamic Understanding of User Cognition and Decision-Making
Once materials can be called upon, the next question the system faces is: what does the same medical knowledge mean for different audiences?
Traditional audience segmentation usually remains at the categorical level—doctors vs. patients, specialists vs. grassroots, urban vs. rural. These classifications can guide channel placements but cannot answer: when an evidence-based doctor and a clinically experience-oriented doctor receive the same disease cognition, which expressions are more likely to influence their judgment, and which will be overlooked.
Based on the medical communication context, the system generates AI Personas for different communication targets. The team can directly interact with these Personas, observing how different groups accept information along real communication paths: which evidence more easily establishes long-term trust with evidence-based doctors, which expressions are more likely to reduce anxiety for risk-averse patients, and which content formats are more likely to generate follow-up discussions in conference settings.
Thus, medical communication shifts from material adaptation to the design capability of cognitive pathways.
Cross-Channel Multimodal Content Expression, Communication Paths Settled as System Model Capabilities
Once cognitive paths are clarified, the system can continuously and automatically generate cross-channel expressions. The same medical theme can simultaneously output academic communication content for doctors, popular science content for patients, conference communication materials, and digital platform content versions—without needing to restart a content project for each communication. The communication team shifts from executing rewriting tasks to observing and adjusting content performance across different paths.
This represents a structural change in content production methods: from phase-based production to a continuous operational capability for content growth.
The project ultimately helps the team identify three core communication paths: evidence-based trust-building paths, risk understanding paths, and long-term management cognition paths. These judgments do not disappear with the end of the communication project but instead settle into a medical communication model that the enterprise can continuously call upon—and enter the next round of disease education communication strategy design.

Medical content production has always been a necessary investment for healthcare companies. However, there has always been a gap between it and "sustained cognitive influence." This gap is a problem of communication structure, not production efficiency.
The changes brought by GEA are not just about improving content production efficiency but represent a structural change in medical communication methods. In the past, medical content production typically occurred before communication nodes, serving as a phase preparation step; now, it has become a continuous capability that runs throughout the entire disease education process.
When medical knowledge can continuously operate, accumulate, and adapt to different audience cognitive paths within the system, it truly transforms from one-time content output into a communication capability that enterprises can rely on long-term.
If you have similar scenario needs, feel free to scan the code to schedule a corporate diagnosis.

Category
Pharma
Date
2026-06-12
Read Time
5 min read
Share Page
Related Recommendations
Leading Digital Healthcare: The Pharmaceutical Industry's GEA Strategy Launch, Opening a New Paradigm for Pharmaceutical Academic Operations with System Capabilities | Tezign x unimind
